Medication Prior Authorization: The Complete 2026 Guide for Medical Clinics
If you run a medical clinic in the USA, manage a community medical center, or operate a family medical center, you already know the struggle. You diagnose a patient, write a prescription, and then, silence. The pharmacy calls back: “Insurance won’t cover it.”
Behind every prescription is a billing reality: Insurance approval complexity.
When medication prior authorization is poorly managed, your reimbursement slows down—or stops entirely. And with search demand for specific medications exploding across the United States, this administrative hurdle is affecting more patients than ever.
Let’s look at what people are actually searching for right now:
| Medication Keyword | Monthly Search Volume |
|---|---|
| ADHD Medication | 135,000 |
| Anxiety Medication | 110,000 |
| Nausea Medication | 40,500 |
| Gout Medication | 40,500 |
| High Blood Pressure Medication | 33,100 |
| Migraine Medication | 33,100 |
| Depression Medication | 27,100 |
| Thyroid Medication | 22,200 |
| Herpes Medication | 22,200 |
| Bipolar Medication | 18,100 |
| Acne Medication | 14,800 |
Millions of Americans are searching for these terms every month. They need help. But when they finally visit your medical clinic near me, the last thing they expect is to wait days or weeks for their insurance to approve the medication you just prescribed.
In this guide, we’re going to break down medication prior authorization in a way that’s clear, practical, and immediately useful. Think of me as your friendly tutor walking you through the maze.
What Is Medication Prior Authorization? (Let’s Start Simple)
Imagine you’re a manager at a company, and an employee wants to buy a new $2,000 laptop using the company credit card. You’d probably want to approve it first, right? You’d ask: “Do they really need it? Is there a cheaper option?”
Medication prior authorization is exactly that. It’s a requirement from medical insurance providers that forces the clinic to obtain approval before a prescription is covered by the plan .
This is most common with:
- Controlled substances (like ADHD medication)
- Psychiatric medications (anxiety medication, depression medication, bipolar medication)
- Long-term chronic treatments (thyroid medication, high blood pressure medication)
- Specialty drugs (like GLP-1s for diabetes or weight loss)
If approval is not obtained before submission:
❌ The claim gets denied
❌ Payment is delayed by weeks or months
❌ Your staff spends hours on rework—calling insurance, faxing forms, following up
According to the Centers for Medicare & Medicaid Services (CMS) , Medicare and Medicaid plans use structured drug coverage rules that vary by plan and state. You can review the official CMS drug coverage overview here: CMS Drug Coverage Overview.
The Electronic Code of Federal Regulations (eCFR) outlines specific requirements for Medicaid prior authorization, including the new 2026 timelines for decision-making . These regulations are legally binding and give you leverage when dealing with payers.
But here’s the kicker: Most prior authorizations eventually get approved. Data from KFF and the American Medical Association shows that 83% of appealed denials are overturned when properly challenged . The problem isn’t that insurers say no forever—it’s that they delay, frustrate, and hope you give up.
Why Medication Claims Get Denied in the USA
Let’s simplify this. Most denials happen because of one of these five reasons:
1️⃣ Missing Documentation
Insurance companies require proof of medical necessity. If your chart notes don’t clearly justify the medication—like why this specific drug, at this dose, for this patient—the denial risk increases significantly. According to industry data, 31% of prior authorization denials are due to lack of medical necessity documentation .
2️⃣ Step Therapy Not Documented
Many Medicare Advantage Plans and commercial insurers require trying a lower-cost drug first. If that “step” isn’t documented in the patient’s history, the approval is rejected automatically.
3️⃣ Medicaid Formulary Mismatch
Medicaid programs differ by state. Each state has its own drug formulary. If you prescribe a medication that isn’t on that specific state’s approved list, it will be denied—even if it’s the best clinical choice.
Official Resource: Check your state’s specific Medicaid requirements. The Federal Register published the final rule for Contract Year 2026 Medicare Advantage and Part D programs, which includes critical updates to drug coverage requirements . You can access the full text here: CMS CY 2026 Final Rule
4️⃣ Incorrect Medical Terminology Coding
Using inaccurate medical terminology during billing data entry can misclassify the medication. This is where strong internal medicine billing services matter. A simple coding error can trigger a denial that takes weeks to unravel. Approximately 18% of denials stem from incorrect coding or code-diagnosis mismatches .
5️⃣ The “Payer Just Says No” Problem
Sometimes, denials happen simply because the insurance company is playing the odds. They know that many providers won’t appeal. Data shows that Medicare Advantage plans deny about 6.4% of prior authorization requests, but when providers appeal, they win 83% of the time .
Medicaid vs Medicare Advantage: Why Approval Rules Differ
Understanding payer differences is absolutely critical. Let’s break it down simply:
If your front desk doesn’t verify coverage correctly before the patient leaves, the claim gets delayed. Period.
The 2026 Regulatory Overhaul: Both Medicaid and Medicare Advantage are subject to new federal requirements taking effect January 1, 2026. Under the CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) :
- Standard requests must be decided within 7 calendar days
- Expedited requests must be decided within 72 hours
- Payers must provide specific denial reasons, no more vague form letters
- Public reporting of prior authorization metrics begins March 31, 2026
The Mass.gov website provides detailed information about how these changes are being implemented at the state level, including updates to prior authorization processes and metrics reporting .
For a full breakdown of these payer differences, read our dedicated guide:
[Medicaid, Medicare Advantage & Medical Insurance Billing in the USA] (Internal Link to Blog 3)
The Medications That Trigger Prior Auth Most Often
Based on search demand and industry data, these are the high-volume medications that frequently require authorization in internal medicine practices:
- ADHD medication (135,000 monthly searches)
- Anxiety medication (110,000 monthly searches)
- Depression medication (27,100 monthly searches)
- Bipolar medication (18,100 monthly searches)
- Thyroid medication (22,200 monthly searches)
- High blood pressure medication (33,100 monthly searches)
- Migraine medication (33,100 monthly searches)
- Gout medication (40,500 monthly searches)
- Herpes medication (22,200 monthly searches)
- Acne medication (14,800 monthly searches)
Patients searching for a medical clinic near me often don’t realize how much backend insurance work happens before their medication is approved. That’s why your clinical documentation and your internal medicine billing services must be tightly integrated.
How Medication Prior Authorization Impacts Patient RCM
Patient Revenue Cycle Management (RCM) isn’t just about submitting claims. It’s the entire financial journey of a patient, from scheduling to final payment.
When medication prior authorization is delayed, here’s what happens to your RCM:
1. Delays in Care = Delays in Billing
If prior authorization takes too long, the treatment is delayed. That means billing is delayed. The longer it takes to get approval, the longer you wait to get paid.
2. More Denied Claims
Missing prior authorization is one of the top reasons claims get denied. Each denial represents revenue you have to fight for or write off.
3. Higher Administrative Costs
Your staff spends hours on the phone with insurance companies, filling out forms, and tracking statuses. The AMA reports that practices complete an average of 39 prior authorization requests per physician, per week, spending about 13 hours on this task alone . Nearly 40% of practices have staff who work exclusively on prior authorization .
4. Increased Rework and Follow-Up
When something goes wrong, missing info, wrong code, expired approval—your staff has to fix it, resubmit, or appeal. This is pure waste.
5. Unhappy Patients
Patients don’t understand why their anxiety medication isn’t covered. They just know they went to the pharmacy and left empty-handed. This erodes trust and can drive them to another provider.
6. Slower Cash Flow
All of these factors combine to slow down your payments. Your Accounts Receivable (AR) days increase, and your cash flow becomes unpredictable. Strong RCM connects front-desk verification with backend billing follow-up. When these are disconnected, you bleed revenue.
To understand the full RCM ecosystem, read:
[Internal Medicine Billing Services 2026]
The True Cost of Prior Authorization (It’s Worse Than You Think)
Most clinic owners underestimate the financial drag of prior authorization. Let’s look at the real numbers:
- National Volume: Medicare Advantage plans alone processed over 50 million prior authorization requests in 2023
- Denial Rate: Medicare Advantage plans deny approximately 6.4% of requests, resulting in over 3.2 million denials annually
- Appeal Success: 83% of appealed denials are overturned, showing that most denials were inappropriate to begin with
- Per-Physician Cost: For primary care physicians, prior authorization costs between $2,161 and $3,430 annually per doctor in lost time
- Hidden Costs: 40% of physicians have staff who work exclusively on prior authorization
- Patient Abandonment: About 40% of prescriptions delayed by manual prior authorization processes are abandoned by patients entirely
- Provider Frustration: 93% of physicians report that prior authorization delays care
What’s Changing in 2026: The CMS Overhaul
Here’s some good news: 2026 is a landmark year for prior authorization reform.
The CMS Interoperability and Prior Authorization Final Rule (CMS-0057-F) introduces major changes effective January 1, 2026 :
Faster Turnaround Times
- Expedited requests: Decisions within 72 hours
- Standard requests: Decisions within 7 calendar days
- Requests can be extended by up to 14 days if additional information is needed
Transparency Requirements
- Payers must provide specific, detailed denial reasons—including the clinical criteria used
- Public reporting of prior authorization metrics begins March 31, 2026
- Reported metrics include approval rates, denial rates, processing times, and appeal outcomes
Electronic Processing Requirements
- Payers must implement FHIR-based APIs for electronic submission and decision delivery
- By January 2027, 80% of electronic prior authorizations with complete documentation must be answered in real-time
- Provider Access APIs enable retrieval of patient claims and PA data
These rules apply to Medicare Advantage, Medicaid, CHIP, and Qualified Health Plans on the federal exchange . The eCFR has codified these requirements at 42 CFR § 440.230(e) , which now includes the specific timeframes and reporting obligations for state Medicaid agencies . The Workgroup for Electronic Data Interchange (WEDI) provides ongoing updates on these federal requirements, including CMS’s metrics reporting templates for impacted payers .
Industry Commitments
In addition to federal requirements, nearly 50 major insurers representing 270 million Americans have made voluntary commitments to streamline prior authorization. The Blue Cross Blue Shield Association and AHIP are leading this initiative, which includes:
- Honoring existing authorizations for 90 days when patients switch plans
- Clearer denial explanations and appeal guidance
- Working toward real-time electronic approvals by 2027

How Automation Is Fixing Prior Authorization in 2026
Modern medical software companies are rolling out tools that make prior authorization faster and less painful. The Assistant Secretary for Technology Policy (ASTP) reports that 71% of hospitals now use predictive AI integrated into their electronic health records.
Real-World Results
- Electronic submission significantly reduces processing time
- Real-time eligibility verification prevents denials before they happen
- Automated tracking reduces phone calls and follow-up time
- AI-powered documentation helps ensure medical necessity is properly documented
The National Institute of Standards and Technology (NIST) has also published new data exchange algorithms to help protect healthcare data, including recommendations for key-encapsulation mechanisms that secure electronic prior authorization transmissions.
The Bottom Line on Automation
Technology supports humans, it doesn’t replace strategy. You still need accurate documentation, proper medical terminology, and Medicaid rule awareness. But automation can handle the heavy lifting of data gathering and submission.
How Much Does Prior Authorization Support Cost?
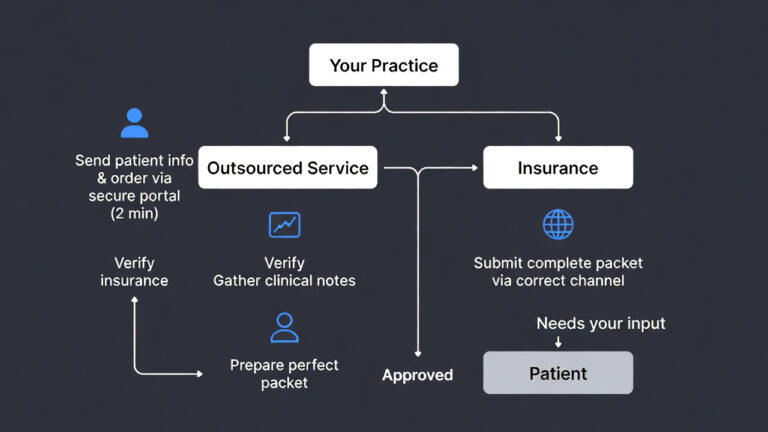
If you’re considering outsourcing this headache, here are typical pricing models for small internal medicine clinics (3–7 providers):
| Model | Typical Cost |
|---|---|
| Per-Authorization | $8–$18 per approval |
| Monthly Flat Support | $1,200–$3,500 per month |
| Bundled RCM Model | 4–8% of collections |
But here’s the better question: How much revenue are you losing right now due to unapproved medications?
Most clinics lose 5–10% of potential reimbursement due to authorization errors. With denial rates averaging 6.4% in Medicare Advantage alone , the financial impact adds up quickly. Outsourcing structured authorization support often costs less than denial losses.
Best Practices for Reducing Medication Denials
Here’s your practical checklist—use this in your clinic starting tomorrow:
✅ Verify insurance before prescribing — Know what’s covered before you write the script
✅ Confirm Medicaid eligibility — Check it’s active for the correct state
✅ Check formulary status — Is the drug on the plan’s approved list?
✅ Document medical necessity clearly — Chart notes should tell the full story
✅ Include specific diagnosis codes — ICD-10 codes linked to requested medication
✅ Document failed treatments — Show what’s been tried and why it didn’t work
✅ Submit authorization before dispensing — Don’t let the patient be the messenger
✅ Track approval expiration dates — Set reminders for renewals (6% of denials are for expired auths)
✅ Monitor denial trends monthly — Are you getting denied for the same reason repeatedly?
✅ Use electronic prior authorization (ePA) where available — It’s faster and tracks better
✅ Train staff on specific payer rules — Medicare Advantage is different from Medicaid
✅ Appeal denials promptly — 83% of denials are overturned on appeal when properly managed
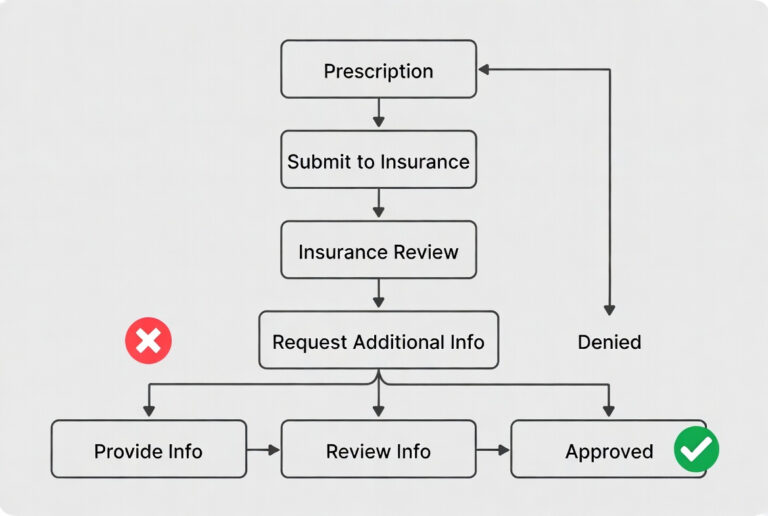
The Appeals Process: When You Get a Denial
Even with the best processes, denials happen. Here’s your five-step roadmap to turn denials into approvals :
Step 1: Deconstruct the Denial Letter
Read it carefully. What’s the specific reason? What’s the deadline? (Typically 30-180 days). Categorize it as administrative (typo, wrong code) or clinical (insufficient justification). Beginning in 2026, payers must provide specific, actionable reasons under the new CMS rules .
Step 2: Build a Robust Appeal Package
Gather updated clinical notes, lab results, and prior treatment history. Write a detailed Letter of Medical Necessity that refutes the denial reason with patient-specific evidence. Include peer-reviewed literature if needed.
Step 3: Navigate the Multi-Level Process
Most appeals succeed at Level 1 (internal review). If denied, escalate to Level 2 (external review by an independent organization). Request a peer-to-peer review, direct conversation with the payer’s medical director—which often resolves disputes quickly .
Step 4: Submit and Follow Up
Submit promptly via the payer’s preferred method. Track status. Follow up regularly. Don’t let it fall through the cracks.
Step 5: Learn from Outcomes
Analyze trends. If documentation issues are frequent, update your checklists. If a specific payer has high denial rates, consider negotiating clearer guidelines.
Pro Tip: Use the appeal letter template available from resources like PatientNotes.ai to structure your appeals effectively .
Final Thoughts: Prior Authorization Is Revenue Protection
Let’s bring this home.
Medication prior authorization in the USA isn’t just an administrative task. It’s a revenue protection system.
If your medical clinic does not have structured processes for:
- ADHD medication approvals
- Anxiety medication insurance checks
- Thyroid medication coverage verification
- Medicaid drug authorization
- Medicare Advantage prescription rules
…you will continue to see silent revenue leakage. Patients will get frustrated. Staff will burn out. Cash flow will suffer.
The solution is integration:
Medication + Insurance + Documentation + Internal Medicine Billing Services + Patient RCM
When these work together, denial rates drop, approvals speed up, and cash flow stabilizes.
Key External Resources
| Resource | Description | Link |
|---|---|---|
| CMS Drug Coverage Overview | Official Medicare drug coverage rules | cms.gov/Medicare/Prescription-Drug-Coverage |
| Medicaid.gov | State-specific Medicaid formularies and rules | medicaid.gov |
| CMS CY 2026 Final Rule | Federal Register – Contract Year 2026 Medicare Advantage and Part D Final Rule | federalregister.gov |
| eCFR § 440.230 | Electronic Code of Federal Regulations – Medicaid prior authorization requirements | ecfr.gov |
| Mass.gov – Prior Authorization Changes | State-level implementation of CMS prior authorization rules | mass.gov/info-details/prior-authorization-process-changes-and-metrics |
| WEDI Federal Update | Workgroup for Electronic Data Interchange – Latest federal updates on prior authorization | wedi.org |
| BCBS Prior Authorization Guide | Blue Cross Blue Shield – Industry commitments and 2026 changes | bcbs.com/news-and-insights/article/simplifying-prior-authorization |
Ready to Master Your Medical Billing?
This guide is Blog 2 in our 4-part series on medical billing and revenue cycle management.
Blog 1 (Main Pillar): [Internal Medicine Billing Services in the USA: 2026 Revenue, Medicaid & Patient RCM Growth Guide]
Blog 3 (Coming Soon): [Medicaid, Medicare Advantage & Medical Insurance Billing in the USA]
Blog 4 (Coming Soon): [Starting a Medical Billing Business in the USA]